
{kind=link}
Prologue
A stroke can strike without warning, suddenly changing the course of a person’s life. One moment, everything is fine; the next, simple tasks like walking, speaking, or remembering a name can become difficult or even impossible. Every year, more than 12 million people experience this kind of disruption, and while stroke is often seen as something that happens to older adults, it is increasingly affecting younger people, especially in parts of the world with limited access to healthcare.
The good news? Our understanding of the brain is catching up with the challenge. Scientists have discovered that the brain is far more adaptable than previously believed. Through a process called neuroplasticity, the brain can reorganize itself, forming new connections and finding new ways to carry out tasks that may have been lost after a stroke. This ability is the foundation for modern stroke rehabilitation.
Rehabilitation is no longer just about learning to cope — it’s about helping the brain recover and rewire. With the support of dedicated therapy teams and emerging technologies like robotics, brain-computer interfaces, and virtual reality, stroke survivors today have more tools than ever to regain independence and quality of life.
This article explores what happens to the brain during a stroke, the types of impairment it can cause, and how rehabilitation works to restore function. We will look at traditional therapies as well as exciting new approaches like robotics, brain-computer interfaces, and virtual reality. Grounded in science, but written for curious minds, this is a guide to understanding stroke and the powerful tools that are helping survivors rebuild their lives.
Introduction
Stroke is a major global health issue, causing millions of deaths and significant disability each year. In 2023, the Global Burden of Disease study ranked neurological disorders (including stroke) as a major global health issue. Stroke increases with age; more than 60% of strokes occur in people under 70 years of age, and 16% affect those under 50. Alarmingly, stroke rates are rising fastest in low- and middle-income countries. One in four people over age 25 will experience a stroke in their lifetime, with over 12 million new cases annually.
A stroke occurs when the blood flow to the brain is disrupted, either by a blockage (ischemic stroke) or rupture (hemorrhagic stroke) of blood vessels. This interruption in blood flow causes brain cells to become damaged or die, leading to many impairments. These impairments can vary depending on the location and severity of the stroke and can affect many aspects of a person’s abilities, including movement, speech, cognition, and sensory perception.
There are two main types of strokes:
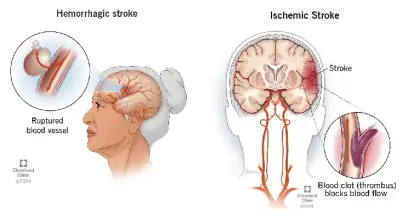
- Hemorrhagic stroke (13%): This happens when a blood vessel in the brain bursts and bleeds into the surrounding area.
- Ischemic stroke (87%): This is the most common kind. It happens when a blood clot blocks a blood vessel in the brain.
There is another type of stroke commonly known as mini stroke:
- TIA (transient ischemic attack/mini stroke): Here, the symptoms go away on their own, but it is still a warning sign of a possible major stroke in the future.
Some people recover fully, while others may have long-term effects. Around 101 million people worldwide live with the long-term effects of stroke, and the consequences can be life-altering, affecting movement, speech, eating, emotions, and thinking. Rehabilitation is essential for recovery, helping people regain function and improve their quality of life.
Rehabilitation Medicine
Rehabilitation medicine, also known as Physical Medicine and Rehabilitation or physiatry, focuses on restoring and enhancing functional ability and quality of life for people with physical impairments or disabilities resulting from illness or injury.

Rehabilitation medicine involves a multidisciplinary or interdisciplinary approach. In addition to the rehabilitation medicine physician, the team includes nurses, members of physical therapy, occupational therapy, speech therapy, and other therapies to address specific needs and improve function.
What Happens in the Brain During a Stroke?
The brain is overly complex and its functions are often spread across multiple regions. Therefore, impairments following a stroke depend on the location and extent of the brain damage. The brain is divided into several regions, each responsible for different functions. For example, the frontal lobe controls movement, speech, and executive functions, while the temporal lobe engages in memory and language understanding. When a stroke damages a particular area of the brain, the functions controlled by that region can be impaired.
Types of Stroke Impairments
Stroke impairments can be classified into several categories, including motor impairments, cognitive impairments, sensory impairments, and speech and language impairments. The exact nature and severity of these impairments vary from person to person, depending on the size and location of the stroke.
Motor Impairments
Motor impairments are among the most common consequences of a stroke, as the areas of motor control of the brain are often affected.
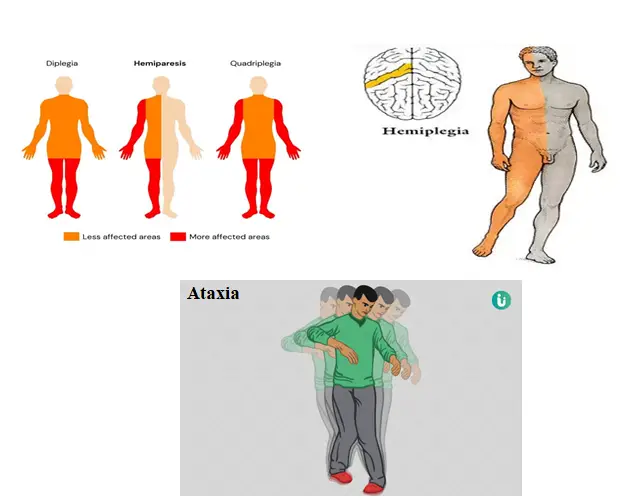
Motor impairments can include weakness (hemiparesis), paralysis (hemiplegia), lack of coordination, and balance problems. These impairments are usually seen on one side of the body, opposite to the side of the brain affected by the stroke.
- Hemiparesis refers to weakness on one side of the body. The severity can range from mild weakness to complete loss of strength in the arm, leg, or both. In severe cases, individuals may have difficulty walking, lifting objects, or performing basic tasks like brushing their teeth.
- Hemiplegia is a more severe condition than hemiparesis, involving complete paralysis of one side of the body. This typically requires intensive rehabilitation to regain some degree of movement and independence.
- Ataxia is another form of motor impairment that affects coordination and balance. This may lead to difficulty walking, maintaining posture, or performing fine motor tasks (like buttoning a shirt).
These motor impairments are linked to damage in brain areas responsible for movement control. For example, the motor cortex in the frontal lobe plays a critical role in voluntary movements. Damage to this area can impair the brain’s ability to send motor signals to the muscles.
Cognitive Impairments
Cognitive impairments are common in stroke survivors, particularly when the stroke affects areas of the brain involved in thinking, memory, and problem-solving. The brain’s frontal lobe, parietal lobe, and temporal lobe are particularly critical in these functions see Fig. e).

Cognitive impairments can vary widely and may include the following:
- Memory loss: Many stroke survivors experience difficulties with short-term and long-term memory. This can make it challenging to remember recent events or recall learned information.
- Attention and concentration issues: People who have had a stroke may find it difficult to focus on tasks for extended periods, leading to distractibility and poor task completion.
- Executive dysfunction: The executive functions of the brain, which involve planning, decision-making, and organizing, can be disrupted. This can lead to difficulties in managing daily tasks, making decisions, or setting goals.
- Difficulty with problem-solving: Stroke survivors may experience challenges in solving complex problems or finding creative solutions to everyday issues. This can impair both personal and professional life.
These cognitive deficits are often linked to damage in the prefrontal cortex, an area of the brain responsible for higher-order functions such as decision-making and planning, as well as the hippocampus, which is involved in memory formation.
Sensory Impairments
Sensory impairments are another common result of stroke. These impairments occur when the stroke damages areas of the brain responsible for processing sensory information. Sensory impairments can affect the senses of touch, sight, hearing, and taste (see Fig. f).
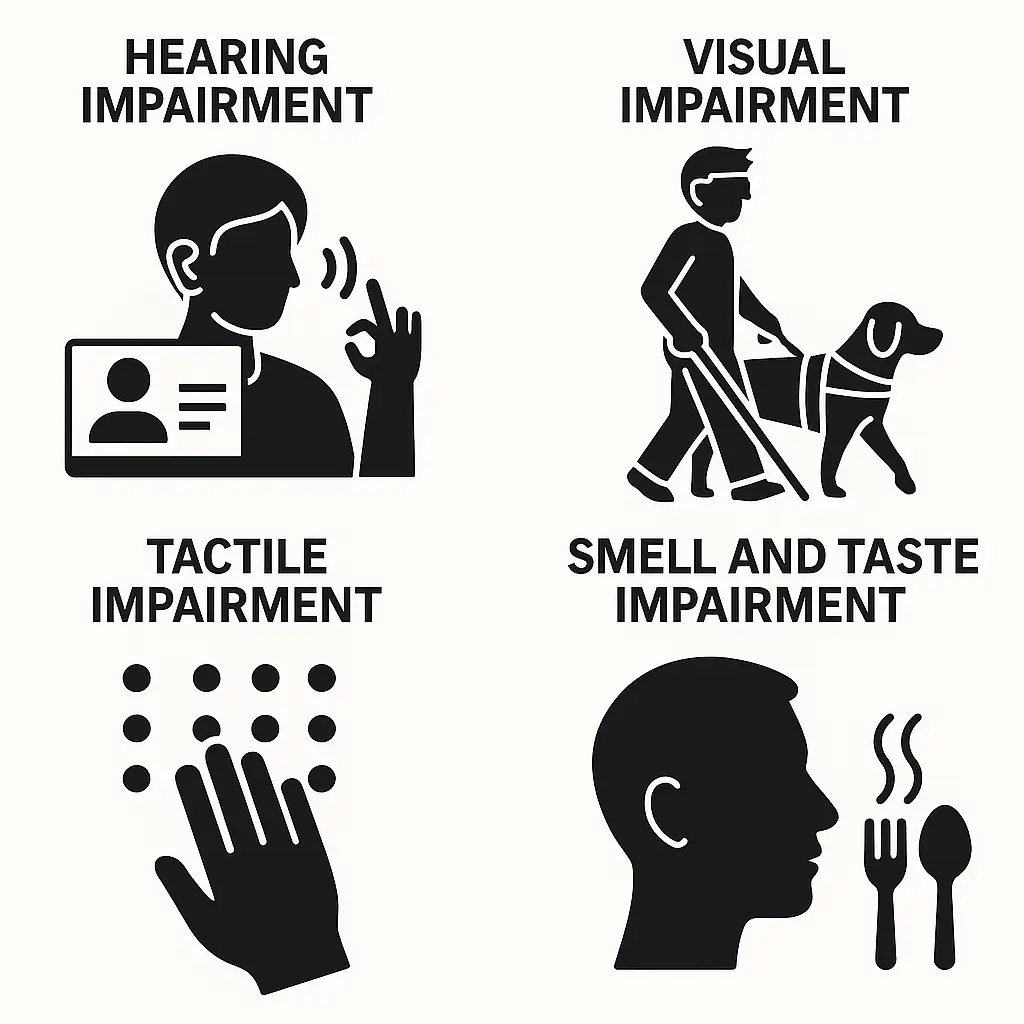
- Touch: Many stroke survivors experience altered sensations, such as numbness, tingling, or heightened sensitivity (paraesthesia). This can make it difficult to feel the texture of objects or determine their position in space.
- Visual disturbances: Damage to the brain’s occipital lobe, which processes visual information, can lead to a variety of visual impairments, such as hemianopia (blindness in one-half of the visual field) or visual neglect (a failure to address objects in one part of the visual field).
- Hearing loss: While less common, strokes affecting the auditory cortex or other parts of the brain that process sound can lead to hearing impairments.
- Taste and smell: A stroke can also affect the brain’s ability to process taste and smell. This may result in loss of taste (ageusia) or altered taste perception (dysgeusia), as well as loss of smell (anosmia).
These impairments are related to the damage of specific sensory regions in the brain, such as the somatosensory cortex (for touch) or the auditory cortex (for sound).
Speech and Language Impairments
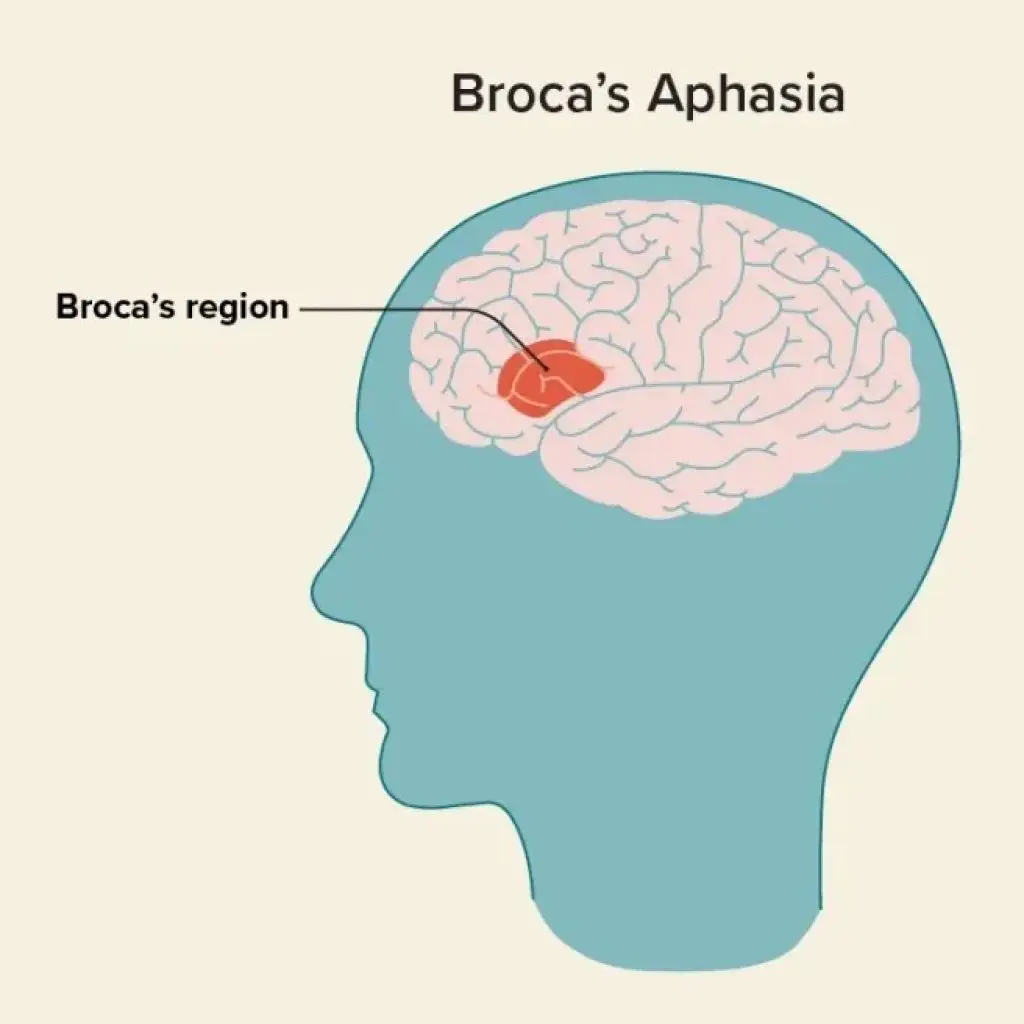
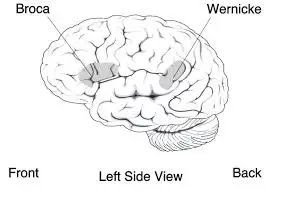
Speech and language problems are common after a stroke, especially when the stroke affects areas of the brain involved in language processing. Aphasia is the most common speech and language disorder resulting from a stroke. Aphasia can affect a person’s ability to speak, understand speech, read, and write.
- Broca’s aphasia: Results from damage to Broca’s area in the frontal lobe, which controls speech production. Individuals with Broca’s aphasia may have difficulty speaking clearly, but their comprehension remains relatively intact.
- Wernicke’s aphasia: Damage to the temporal lobe can cause Wernicke’s aphasia (Figure 8), where individuals have difficulty understanding language and may produce fluent but meaningless speech.
- Global aphasia: This is a severe form of aphasia that affects both speaking and understanding language. It often results from widespread damage to the language centres of the brain.
Strokes that affect the cerebellum or brainstem may also lead to speech problems, such as dysarthria, which causes slurred or unclear speech due to muscle weakness.
Emotional and Behavioural Changes
Stroke survivors often experience emotional and behavioural changes due to the brain’s disruption of emotional regulation centres. These changes can include the following.
- Depression: It is common for stroke survivors to experience depression due to the sudden changes in their physical and cognitive abilities. Depression can make rehabilitation more challenging.
- Anxiety: Many stroke survivors develop anxiety, particularly related to the fear of another stroke or the loss of independence.
- Personality changes: Strokes affecting the frontal lobes can result in changes in personality, such as impulsivity, irritability, or apathy.
These emotional and behavioural changes are often linked to damage to the limbic system or prefrontal cortex, which play key roles in emotion regulation and social behaviour.
The Science of Stroke Rehabilitation- Neuroplasticity: The Brain’s Ability to Adapt
One of the most powerful concepts in stroke rehabilitation is neuroplasticity. Stroke rehabilitation is grounded in the science of neuroplasticity, which is the incredible ability of the brain to change and reorganize itself by forming new connections (rewiring) between neurons (brain cells). This process is essential for learning, memory, and recovery after brain injuries like a stroke. When a stroke occurs, it can damage certain areas of the brain, disrupting the pathways that control vital functions like movement, speech, and cognitive abilities. However, the brain does not give up; it can rewire itself by creating new neural pathways, finding alternative routes to perform the lost functions. Over time, this neuroplasticity can allow stroke survivors to regain lost abilities, although the extent of recovery depends on factors such as the severity of the stroke, the area of the brain affected, and how quickly rehabilitation begins. Rehabilitation uses this principle by engaging patients in targeted physical, occupational, and speech therapies to help retrain the brain and body. Techniques such as task-specific training, constraint-induced movement therapy, and neuromodulation aim to stimulate recovery and improve functional outcomes. The earlier and more intensive the rehabilitation, the better the chances for meaningful recovery, although progress can continue even months or years after a stroke.
Neuroplasticity occurs through two main processes: functional reorganization and structural changes. Functional reorganization refers to the brain’s ability to recruit and repurpose other regions to perform tasks previously managed by the damaged areas. For instance, if a stroke affects the motor cortex responsible for hand movements, nearby regions may take on some of those motor control functions. Structural changes involve physical changes in the wiring of the brain, such as the creation of new synapses (connections between neurons), which allow for improved communication between regions of the brain.
This neuroplastic potential is influenced by various factors, including the timing and intensity of rehabilitation, the type of therapy used, and the patient’s age, as younger individuals tend to experience more significant neuroplastic changes. Rehabilitation interventions harness this process by engaging patients in targeted exercises, activities, and tasks that encourage the brain to reorganize and form new neural pathways. Neuroplasticity is driven by practice and effort. When a stroke survivor works on exercises or tasks, the brain gets a chance to “rewire” itself, creating new neural pathways. Younger people tend to experience more dramatic changes in their brains after a stroke, but people of all ages can benefit from rehab and encourage their brains to reorganize.
Key Approaches to Stroke Rehabilitation
Stroke rehabilitation involves a range of therapies designed to address different aspects of impairment caused by a stroke. The most commonly used rehabilitation strategies are physical therapy, occupational therapy, and speech therapy.
- Physical Therapy (PT): Physical therapy focuses on improving the patient’s movement and strength, particularly in the limbs affected by the stroke. After a stroke, patients often experience paralysis or weakness (hemiparesis) on one side of their body.

Physical therapists use various exercises and techniques to help restore mobility, strength, and coordination. One common approach is task-specific training, where patients practice functional movements and activities that mimic real-life tasks (e.g., walking, reaching, or climbing stairs). This helps reinforce motor control and improves independence. In addition, constraint-induced movement therapy (CIMT) has been used successfully, which involves constraining the unaffected limb and encouraging the patient to use the affected limb more frequently. This technique forces the brain to reorganize and improve the motor function of the weaker side of the body.
- Occupational Therapy (OT): Occupational therapy helps stroke survivors regain the skills necessary for daily living activities, such as dressing, cooking, and bathing. OT focuses on improving fine motor skills, hand-eye coordination, and cognitive functions. Since strokes often result in difficulties with grasping, holding, or manipulating objects, occupational therapists work with patients on exercises that simulate daily tasks.

This therapy also helps patients adapt to changes in their environment, using assistive devices such as grab bars or modified kitchen tools to increase independence. Cognitive rehabilitation is a subfield of occupational therapy/speech pathology that addresses the cognitive impairments associated with stroke, including memory, attention, and problem-solving difficulties. Cognitive exercises and strategies, such as memory aids or structured routines, are often employed to help patients regain their cognitive functioning.
- Speech Therapy: Speech therapists assess the type and severity of aphasia and provide individualized strategies to improve communication. Speech therapy techniques include language exercises, where patients work on repeating words or sentences, as well as semantic training, which helps them understand and use words correctly in context.

In addition, some stroke survivors develop dysphagia, which makes swallowing difficult and increases the risk of choking. Speech therapists work with these patients to improve swallowing techniques, making eating and drinking safer and more comfortable.
Innovative Approaches and Technologies in Stroke Rehabilitation
In recent years, advancements in technology have led to the development of more sophisticated tools for stroke rehabilitation. These technologies aim to complement traditional therapies by providing additional support for patients and improving the rehabilitation process.

Orthotics play a crucial role in stroke rehabilitation by providing support, alignment, and stability to affected limbs, particularly the lower extremities.
They help manage muscle weakness, spasticity, and joint instability, often seen after a stroke. Devices like ankle-foot orthoses (AFO), including the functional electrical system (FES), can improve gait, balance, and mobility, allowing patients to participate more effectively in physical therapy and daily activities.

Robotic devices are increasingly used in physical therapy to assist with repetitive exercises. These robots can guide the patient’s movements, providing both physical support and feedback during exercises.
Robotic systems can also be programmed to provide precise, tailored exercises that challenge the patient’s specific impairments. Research has shown that robotic therapy can improve motor function and encourage neuroplasticity by helping patients perform movements that would be difficult or impossible otherwise.
Virtual Reality (VR) and Augmented Reality (AR):
Virtual reality and augmented reality are also being utilized in stroke rehabilitation to provide immersive and engaging therapy. VR systems allow patients to participate in simulated environments where they can practice motor tasks, such as reaching or walking while receiving real-time feedback. These systems have been shown to improve motor skills and increase motivation, particularly in patients with severe impairments. Similarly, AR uses technology to overlay digital information onto the real world, helping patients improve motor control and coordination by interacting with virtual objects in their environment.
Transcranial Magnetic Stimulation (TMS)
Transcranial magnetic stimulation is a non-invasive technique that uses magnetic fields to stimulate specific areas of the brain. In stroke rehabilitation, TMS can be used to enhance neuroplasticity by targeting the unaffected brain regions, encouraging them to take over functions lost due to the stroke. TMS has shown promise in improving motor function, particularly when combined with physical therapy.
Brain Computer Interface: A Brain-Computer Interface (BCI) is an emerging technology in stroke rehabilitation that enables direct communication between the brain and external devices, bypassing damaged neural pathways. By detecting and interpreting brain signals—often through electroencephalography (EEG)—BCIs can translate a patient’s intention to move into control signals for assistive devices, such as robotic limbs or virtual environments. This feedback-driven therapy enhances neuroplasticity, promoting the reorganization of neural networks and aiding motor recovery. BCIs hold significant promise in restoring movement and improving the quality of life for stroke survivors, especially those with severe motor impairments.
Looking Ahead: Challenges and Future Directions
Challenges
- One major challenge is the timing of rehabilitation. The first few months after a stroke are crucial for maximizing recovery, as this is when the brain is most plastic. However, access to rehabilitation services may be limited due to financial, geographic, or logistical constraints. Efforts are being made to increase accessibility and reduce wait times for therapy.
- Another challenge is that recovery can vary widely between individuals. While some stroke survivors make significant progress, others may face lasting disabilities. Researchers are working to understand the factors that affect recovery, such as the size and location of the stroke and the patient’s age, to create more personalized rehab plans.
Future Directions
As technology continues to advance, the future of stroke rehabilitation looks promising. New therapies, such as robotic devices, virtual reality, and brain stimulation techniques, hold the potential to accelerate recovery and provide more personalized care. Advances in neuroimaging may also allow for better identification of regions in the brain that can be targeted for rehabilitation, improving the precision of therapeutic interventions. Furthermore, advancements in genetic research and personalized medicine could lead to treatments tailored to each individual’s unique brain and recovery needs. As our understanding of the brain and neuroplasticity grows, stroke rehabilitation is likely to become more effective and accessible to a wider range of patients.
Conclusion
Stroke rehabilitation is a complex, multifaceted process that requires a personalized and interdisciplinary approach. Through the combined efforts of physical, occupational, and speech therapists, stroke survivors can experience meaningful improvements in their functional abilities. The science of neuroplasticity plays a central role in stroke recovery, and therapeutic interventions are designed to harness the brain’s ability to reorganize and form new neural connections. As science continues to unlock the secrets of the brain, the future of stroke rehab looks brighter, offering new hope for those recovering from a stroke. With the help of innovative technologies such as robotic therapy, virtual reality, and brain stimulation techniques, stroke rehabilitation is continually evolving, offering hope and enhanced recovery potential for stroke survivors.
References
[1] https://www.stroke.org/en/about-stroke/types-of-stroke/ischemic-stroke-clots, Accessed: 2025-7-12.
[2] Transient ischemic attack, en, https://apsfa.org/transientischemic-attack/, Accessed: 2025-7-12.
[3] Redirect notice, en, https://www.google.com/url?sa=i&url=https : / / www . doctorbe . com / blog / treatment – for – flaccid – paralysis&psig=AOvVaw3UpssZK7R-pAmGTdkVhILp&ust=17525790356500 source=images&cd=vfe&opi=89978449&ved=0CBAQjRxqFwoTCNDmzoKfvI4 Accessed: 2025-7-14.
[4] VA rating for cognitive impairment, en, https://www.stoneroselaw.com/veteranslaw/va-rating-for-cognitive-impairment/, Accessed: 2025-7-13, Apr. 2025.
[5] Sensory impairments illuminated in illustrations, en, https://chatgpt.com/s/m_6874e96717fc819190b977bd71a1baf0, Accessed: 2025-7-14, Jul. 2025.
[6] C. Whelan, Broca’s aphasia: Symptoms, treatments, types,
and outlook, en, https://www.healthline.com/health/brocas-
aphasia, Accessed: 2026-1-20, Aug. 2017.
[7] N. Silver, Wernicke’s aphasia: Symptoms, causes, and treatment, en, https://www.healthline.com/health/wernickesaphasia, Accessed: 2025-7-13, Jun. 2017.20.
[8] Neurological basis for speech and language, en, https : / /www.slideserve.com/adamdaniel/aphasia, Accessed: 2025-7- 13, Mar. 2013.
[9] D. G. Smith, “What to look for in a physical therapist,” NY Times, Mar. 2023.
[10] Occupational therapy, https://www.northshore.org/physicalmedicine-rehabilitation/our-services/occupational-therapy/, Accessed: 2025-7-14, Sep. 2013.
[11] https://www.medicalnewstoday.com/articles/does-medicare-cover-speech-therapy.
[12] What is TMS? How does TMS work? MagVenture TMS therapy, en, Jan. 2020.
[13] Providing adequate training to #healthcareprofessionals is acomplex task, es, https : / / www . linkedin . com / posts / the – games – institute _ healthcareprofessionals – rehabilitation – activity-7208533992126517248-uEZd/, Jun. 2024.